|
|
Post by bugsy on Mar 27, 2008 9:35:49 GMT -5
Thank you to who gave me this article link!  tinyurl.com/2hejkn tinyurl.com/2hejknIllinois State professor excels in biology research Andrew Cross, Daily Vidette Staff Issue date: 3/26/08 Section: News PrintEmail Article Tools Page 1 of 1 Dr. David L. Williams, professor of biological science, and a team of researchers from the National Institutes of Health (NIH) Chemical Genomics Center are looking toward a possible treatment for schistosomiasis, a disease that affects more than 200 million people around the world. Schistosomiasis, also known as snail fever, can cause diarrhea, anemia, organ damage, internal bleeding and death. Individuals are infected with Schistosoma, parasitic worms that cause schistosomiasis, when they come into contact with water inhabited by snails, which act as hosts for the parasite. "There is no human schistosomiasis in North America," Williams said. "There are no suitable snail hosts." But schistosomiasis in humans is found in at least 70 countries around the world, resulting in approximately 280,000 deaths each year. "One of the problems with schistosomiasis is that people can be cured of the infection, but they do not develop immunity to subsequent exposure to the parasite and can be easily reinfected, Williams noted. Using state of the art technology at the NIH Chemical Genomics Center in Rockville Maryland, Williams and his team were able to screen 70,000 compounds against a biochemical pathway from the worm. Developed in 2004, the facilities at the Chemical Genomics Center use "the tools of small molecule discovery to develop chemical probes for the study of protein and cell functions," according to Dr. Anton Simeonov, Group Leader at the NIH. Simeonov went on to say that access to the screening center is allowed by peer review, conducted by an independent panel of experts. "Professor Williams was one of the very first investigators to apply to the network," Simeonov said. Williams believes the next two to three years will be spent developing derivatives of the compounds already identified. "Optimistically, we expect to have compounds in clinical trials for schistosomiasis treatment in four to five years," Williams said. "Funding is now the key factor." Williams and other experts believe praziquantel, the only drug currently on the market to combat schistosomiasis, will lose effectiveness if the parasites are able to adapt to the drug. "Our goal is to use the new drugs in combination with the current drug to prevent drug resistant parasites from evolving," Williams said. ______________________ Faith |
|
|
|
Post by bugsy on Mar 27, 2008 9:49:12 GMT -5
Here is something from the World Health Organization saying which snail genus carries this disease. Link: www.who.int/wormcontrol/statistics/useful_info/en/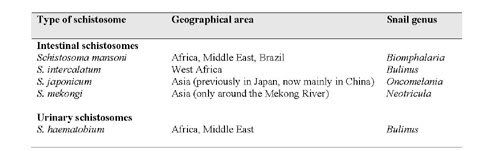 Now they mean to tell me in the first posted article that there is NO WAY that a snail could be in U.S. waters which could carry this disease?!!! An aside, swimmers itch is a mild version of this same disease. It is basically a swimmer's itch which does parasitize a human until treated. We HAVE SNAILS in our lakes in order to contract swimmers itch from this host. Birds poo in water and snails expell this and we swim in it. Are they so closed minded that they really believe that this is not possible and probable. As I become better I am going to be more angry. Faith.....soon to be called Patience...lol |
|
|
|
Post by bugsy on Mar 27, 2008 10:00:56 GMT -5
Here's proof that this snail is indigenous in the U.S. and Europe and Lord knows where else. Here are the snails taken from the above WHO list: Biomphalaria - Supposedly only in Africa, Middle East and Brazil Here is a link where it states it has been in U.S. since the days of the Jurassic Period. tinyurl.com/yw5c76 Scroll down to S197. It is a pdf or I would have cut and pasted. Sorry. "Biomphalaria Snails Importnace & Biological Characterization." _______________________________ Not a concern eh? www.jwildlifedis.org/cgi/reprint/6/4/262.pdfExcerpt: ________________________ Control Methods for Snail-Borne Zoonoses GLENN L. HOFFMAN Eastern Fish Disease Laboratory Bureau Sport Fisheries and Wildlife Leetown (P.O. Kearneysville), W. Va., U.S.A. 25430 Abstract All trematodes which cause infections and diseases in humans (zoonoses) require snails for their first intermediate host. Some have additional intermediate hosts such as crustaceans, fishes and frogs. In this paper I have discussed the use of various procedures for controlling snail populations thereby reducing the population of trematodes whose cercariae penetrate the skin of man, or which are acquired by eating raw aquatic vegetation such as watercress, or which cause pathology in fish. Biological, chemical, and physical snail control techniques are discussed. The most promising molluscucides are copper ýompounds, Bayluscide, biocidal rubber and molluscicidal bait. As far ;s known, all zoonotic trematodes of man require snails as their first. _________________________ Faith |
|
|
|
Post by bugsy on Mar 27, 2008 14:41:17 GMT -5
A bitter pill to swallow. These ducks in Germany are receiving better medical treatment than human beings who are with or without medical insurance. tinyurl.com/yqud9gThe effect of praziquantel on Trichobilharzia (Digenea, Schistosomatidae), a cause of swimmer's dermatitis in humans][Article in German] Müller V, Kimmig P, Frank W. Abteilung für Parasitologie (Institut für Zoologie), Universität Hohenheim, Germany. Cases of swimmer's itch caused by cercariae of the genus Trichobilharzia have spread during the last years in Southwestern Germany and increased in intensity. The only consequence was to forbid swimming because no effective strategies are known which would be ecologically or financially acceptable. In this examination we therefore tried, by means of medication of ducks, the possible final hosts, to kill the different stages of Trichobilharzia in patency and prepatency in order to interrupt the parasitic cycle. For this the effectiveness of praziquantel on the parasitic stages in the final host (preadults, adults, eggs or fully developed miracidia) was tested in experimentally infected dwarf mallards (Anas platyrhynchos, hemerot.) and mallards (Anas platyrhynchos platyrhynchos). During therapy of ducks with patent Trichobilharzia infection, onefold or twofold application of this drug (1 x 500 mg/duck, 1 x 300 mg/duck, 2 x 200 mg/duck) only prevented the releasing of eggs with hatchable miracidia for up to 24 h. Only a threefold application of 200 mg/duck in 24 h intervals led to a permanent reduction of detectable miracidia. Application of praziquantel in low doses (30 or 40 mg per duck and day) did not reduce the number of released miracidia. Medication with praziquantel led to a strong shift of adult worms located in the enteric veins of the ducks to the liver veins in a little as 3 h; examinations by scanning electron microscopy revealed changes in the worms' surface and damage of the tegument. During prepatency doses of 22.5 mg praziquantel per duck and day, given continuously for one week, were sufficient to completely stop the release of miracidia. In this low dosage, a special preparation of the bitter drug was voluntarily swallowed by the ducks, thus providing in principal a simple, cheap and ecologically sound method of controlling cercarial dermatitis. PMID: 8220576 [PubMed - indexed for MEDLINE ________________________ So what now? Do we just sit here and let the CDC do NOTHING......let Kaiser do NOTHING....? Am tempted to call the DEQ locally. Not sure. Faith |
|
|
|
Post by shubot on Mar 27, 2008 20:37:55 GMT -5
Hi, Faith.
Thanks for this info eventho it makes me sick. We used to play with snails in the muddy waters in Texas when we were kids! Yes, there are snales here.
shubot
|
|
|
|
Post by 0happyday on Mar 27, 2008 22:56:35 GMT -5
I'm scared to even look at this right now. This was one of my first research projects when trying to find out what was wrong with me.
I'll look tomorrow when I'm not so tired. Night 0happyday
|
|
|
|
Post by bugsy on Mar 28, 2008 12:53:37 GMT -5
Hey, sorry to make you all sick and scared.  If it's any consolation...over 200 million are infected with this and they seem to live with it or cure it somehow. Some become more immune over thousands of years such as the Chinese. I read something the other day that said that they have gotten it under control to about a MILLION infected...a MILLION...OMG. That is a small number to them. It is nature. It has always been here only we just didn't know it. It will be okay. Our gov't just needs to get with the PROGRAM...literally...the snail eradication program. Like Erin Brochovich says "Before they can see the light at the end of the tunnel first they have to admit that there is a tunnel" or some such thing. lol Sooooooooo true. I think we will be okay. I'm normalizing .... contrary to my familys beliefs..hahaha. Sounds funny. But true. Body, skin, eyes, feet, hands.....making a come back. There is definite HOPE on the horizon..with or without the CDC's help.  Faith |
|
|
|
Post by bugsy on Mar 28, 2008 20:57:20 GMT -5
Oh, here we go. Finally something to explain WHY this stuff comes out after the shower. Anyone who has had this at least two years has seen the white fuzz/worm type stuff emerge from unbroken skin upon air drying of skin. I knew there had to be an explaination of this. I found it. This cercaria is viewing US as a sort of non-snail host...only we are NOT always in water and when they try to swim to their new host they hit the air....due to the fact that WE are NOT water beasts but walk on land and then they try to leave for a new host and die....eventually. They do fight for a while don't they..! Here is what I found. __________________________________ www.deq.state.mi.us/documents/deq-water-illm-itchbrochure.pdfAs an individual emerges from the water, the cercariae enter the skin as the body air dries. Faith |
|
|
|
Post by shubot on Mar 28, 2008 22:59:29 GMT -5
Hi, Faith.
Thanks for the info. I think we have several weird things going on in our body all at the same time. Worms, flat worms, Lyme's, nano-batteries, microscopic aliens, nematodes, flies, ect...
I hope it is just these snails tho. I think it would be much easier to treat and prevent than all of the other weird stuff that I do not understand.
shubot
|
|
|
|
Post by bugsy on Mar 30, 2008 4:32:24 GMT -5
You're quite welcome Shubot. I absolutely agree that this is more than one kind of parasite. I was hoping that it was different stages of same thing. But, it is probably best to eradicate one thing at a time. Slowly, gradually...and aggressively. My only wish is that I had begun this in the very beginning. It is easier to control earlier on. One mistake I did make is thinking when my symptoms disappeared was that I was in the clear....follow up at one month, three month and six month intervals is key. Otherwise a person can end up at square one. They lay eggs in intervals...so that is something to consider.
If I planted flower bulbs in the yard intervals they would bloom sporadically just as these do.
Medicine kills mostly adult and larval stages.....so is lengthy process. Me and husband have begun to take a different approach. Not BIG doses of stuff and then nothing. More like moderate doses longer periods. Seems to work better. Then antibiotics due to the bacteria on the dead ones rising to the surface causing sores. This particular one carries Salmonella from what I've read.
The one good thing we read about was that these particular ones can only live for 48 hours without a host in water. Not sure out of water. BUT I would think that the dead ones being released from body may potentally have bacteria on them and would spray house with lysol.
Car, etc.
Faith
|
|
|
|
Post by shubot on Mar 30, 2008 17:38:53 GMT -5
The one thing that I have been doing non stop since Dec 06 is taking Oregabiotic, garlic oil, vitamin C and MSM every day.
I started out with one every 12 hours and began taking one every 24 hours about two weeks ago. I did this because I could not get antibiotics from the doc.
I am afraid to stop because I fear the worst of the symptoms will return.
shubot
|
|
|
|
Post by bugsy on Mar 31, 2008 5:13:46 GMT -5
Good thinking. I forgot to tell you all something VERY important. I know that some do not have access or are not interested in taking anti-parasitics. That's okay. I've gotten my hands on a 2007 Medical Diagnostic book by Lange from the library and there is something said and in the works about using Artemisim or commonly known as "wormwood" to fight this.
I apologize for not remembering to list this!!!!! If anyone does not believe what I say. Visit your library and ask to see that book and look it up for yourselves.
It states:
Page 1534 under Treatments for Schistosomiasis;
"Artemisinin and its derivatives, recently found to be active against the immature and adult forms, are being evaluated for prophylaxis, treatment of early infection, and cotreatment with praziquantel. "
I'm not stopping for anything anymore shubot..it builds back up. You are smart not to stop what is working for you.
Faith
|
|
|
|
Post by bugsy on Apr 1, 2008 14:26:52 GMT -5
Hello again,
I thought I would post a little about what to expect while healing so you know you are going in the right direction and do not panic. This is with praziquantel day 10.
Itching increases dramatically starting at about 3:00 p.m. sometimes sooner.
Benadryl or whatever other antihistamines you have handy are helpful.
I notice some swelling of hands and feet but this went down by morning.
Baking soda baths help. Selsen Blue, Palmolive Oxyclean without bleach dish soap were used to rotate and draw them out.
Early a.m. showers seemed to show more result in Large hairlike structures exiting. I don't know why but this was consistant.
Stay in as long as you can and as hot as you can and they will come out with just gently pressing down with the palm of your hands. Leave the shampoo, or dish soap on closed eyes and scalp and face as long as possible before rinsing.
I started getting a leathery skin on my face which looked and felt like I had a shellfish allergy reaction. I believe due to the die off. This is coming off gradually with black salve balm and bag balm when uncomfortable at bedtime.
My hands have what looks like horrendous paper cuts all over them and then I coat in bag balm to heal. It seems to get worse then better then worse...etc...is the process. I am beginning to get the thick layer of callous off hands and beginning to feel things again. I missed that. Fingertip feeling making a come back.
This can get a bit painful as well, especially when the large structures start leaving deep muscle tissue. I've felt like I have deep bruising in various areas of body. Then it subsides. Taking lots of antioxidants. Nothing fancy just vitamin C, etc. Drinking fruit juice seems to be helpful.
It got way worse and is now getting a whole lot better. Not saying I'm cured by any stretch but on the way in the right direction.
OH almost forgot the sores and odd granules will surface as well.
I've had this for two years. Would imagine everyone is different.
Just sharing what I'm currently experiencing.
All for now
Faith
|
|
|
|
Post by shubot on Apr 1, 2008 22:24:10 GMT -5
Hi, Faith,
Thanks for the info. I also began taking Hyssop Cleans in Oct. 2006 and have not stopped because I feared GI crawlies thing would come back.
shubot
|
|
|
|
Post by bugsy on Apr 2, 2008 8:54:33 GMT -5
BIG NEWS...for me anyway. MUD snails can carry this as well. In the following article it says that aquatic/and SEMI-AQUATIC snails can carry this. So anyplace WET you or pet or any mammal can contract this is conditions are right (bird poo/pee) (infected mammal poo/pee). tinyurl.com/3yajr3__________________________________ The transmission of all three species is based on a complex four-phase cycle which includes the presence of freshwater snails (Figure 9). Eggs expelled in the urine or faeces of an infected person may reach water, where they hatch rapidly into miracidia, a free-swimming brief larval stage. Depending on the species, the miracidia have to find a specific aquatic or SEMI-AQUATIC freshwater snail as intermediate host within 24 hours. _______________________ Here is the rest of the article: Water-based diseases: transmission by aquatic and semi-aquatic snails Schistosomiasis There are three major types of schistosomiasis that affect man: S. haematobium, S. mansoni and 5. japonicum. The disease is caused by female and male trematode worms inhabiting the blood vessels of the urinary bladder (S. haematobium, S. japonicum) or the portal and mesenteric veins (S. mansoni). Typical visible symptoms of schistosomiasis infection are blood in the urine in the case of S. haematobium, and intermittent diarrhoea and faeces containing blood in the case of S. mansoni (Jordan and Webbe, 1982). Although effective chemotherapy is available, the costs per treatment and per caput make it too expensive for many developing countries. The transmission of all three species is based on a complex four-phase cycle which includes the presence of freshwater snails (Figure 9). Eggs expelled in the urine or faeces of an infected person may reach water, where they hatch rapidly into miracidia, a free-swimming brief larval stage. Depending on the species, the miracidia have to find a specific aquatic or semi-aquatic freshwater snail as intermediate host within 24 hours. S. haematobium, S. mansoni and S. japonicum require snails of the genera Bulinus, Biomphalaria and Oncomelania, respectively. Oncomelania are semi-aquatic snails that live part of the time outside water in moist soil or mud. In the snails, the parasites develop within 4 to 6 weeks into cercariae, a second free-swimming larval stage. It is at this stage that they are infectious for man. Snails shed numerous cercariae into the water. These have to find human beings in contact with water in order to penetrate their skin. Having penetrated the skin of the host, the parasites find their way through the veins, heart and lungs to the final organ, there recommencing the cycle with egg production (Jordan and Webbe, 1982). Bionomics of snail intermediate hosts Although individual snail species require a specific physical environment, the variety of aquatic habitats is almost infinite. Marshes and swamps, permanent or temporary ponds and pools, natural or man-made freshwater lakes or reservoirs, seasonal or permanent or slow flowing river streams, irrigation or drainage canals, rice fields and all other types of standing, slow flowing or impounded water are potential snail breeding sites. Generally, the water needs to be shallow, clean or brackish, with little turbidity. The duration of the life cycle depends on water temperatures. The ideal water temperature ranges from 26° C to 28 °C. Snail intermediate hosts of both S. haematobium and S. mansoni show great tolerance regarding pH values (5.3-9), mean water temperatures (18°-30°C) and salinity. Snails are found in shaded water bodies but are also known to be active when exposed to direct sunlight. The shedding of cercariae correlates with day-time and thus the intensity of sunlight. Furthermore, snails have a remarkable capability to survive long periods (5-8 months) in moist sand or mud (aestivation). Their main source of food is organic matter originating from decaying submerged or emerged vegetation, different species of algae, bacteria and fungi. However, both of these aquatic snail species are sensitive to water velocity and water table fluctuations. Tolerable average current speed ranges between 0.0-0.3 m/s (Jobin and Ippen, 1964; Jobin et al., 1984). In natural rivers, snails are generally dislodged due to turbulence and fleeting shear stresses along the transition zone between the embankment vegetation and the river bed sediments, which are their actual habitat zone (Fritsch, 1993). ________________ All for now Faith |
|
|
|
Post by bugsy on Apr 2, 2008 12:27:36 GMT -5
|
|
|
|
Post by bugsy on Apr 3, 2008 3:32:09 GMT -5
Here is a new article from the Washington Post dated April 1, 2008. A good read. tinyurl.com/2mrcezMedical Mysteries A Suspect Diagnosis It Just Didn't Feel Like an Infection Alison Raphael still doesn't know where she picked up the bug that made her sick. (By Juana Arias For The Washington Post) posted yet about this item. Be the first! By Sandra G. Boodman Washington Post Staff Writer Tuesday, April 1, 2008; Page HE01 It was the middle of the night in May 2006 when Alison Raphael, camped out in her daughter's Manhattan sublet, realized she had a problem she could no longer ignore. The faint traces of blood she'd noticed in her urine earlier in the day had become a crimson stream, and the dull ache on the right side of her groin had intensified. A consultant to UNICEF on a quick trip home from a posting in South Africa, Raphael decided to tough it out. After a sleepless night, she headed straight for the emergency room of a nearby hospital, forsaking the excursion in Central Park that she and her daughter had planned. There, Raphael recalled, doctors took turns poking various spots on her abdomen, asking her "on a scale of 1 to 10 how much it hurt." They seemed disappointed, she said, when she kept responding "two." Several hours later, after the results of urine and blood tests came back, Raphael was discharged with a diagnosis of urinary tract infection and a prescription for the powerful antibiotic Cipro. But as Raphael would learn several weeks later, the cause of her problem was not nearly so simple. To readers whose squeamishness trumps their interest in baffling or unusual illnesses: Consider yourselves warned. Before her trip to New York, Raphael, now 62 and living in Takoma Park, had rarely been sick. There were two notable exceptions in the distant past. She had spent months battling giardia, a water-borne gastrointestinal illness. Along with her family, Raphael had become violently ill from water tainted with amoebas shortly after the family's arrival in Latin America, her husband's first assignment as a Foreign Service officer. Water, Raphael would later learn, was implicated in her urinary problem, too. As she left the ER, Raphael doubted she had a bladder infection, because she felt none of the hallmark burning or twinges. On the bus ride back to Washington, she felt steadily worse and realized she was too sick to endure a 23-hour flight back to Pretoria. She delayed her trip and consulted a doctor in Washington. After considering her symptoms and learning that the bloody urine had cleared up, the doctor gave Raphael more Cipro to knock out any residual infection. Feeling better, she flew back to South Africa, where she consulted a urologist. Because bloody urine can have ominous causes, including cancer, the doctor ordered more urine and blood tests. A CT scan revealed a uterine fibroid, a common benign tumor. A South African gynecologist suggested she undergo a complete hysterectomy in case the fibroid was causing the symptoms, advice Raphael and her Washington gynecologist rejected as unnecessary. In June, the urologist called to report that standard blood and urine tests had found nothing suspicious. But less than an hour later, she called back. "Oh, my God," she told Raphael, "another urine test just came back and you have schistosomiasis. " Schistosomiasis (also known as bilharzia, schisto and snail fever) is an infection caused by parasitic worms that are shed by snails in water. These worms penetrate the skin of people who swim, bathe or otherwise come into contact with contaminated water. The parasite invades the blood vessels, producing eggs that migrate to the intestines or bladder. Urinary schistosomiasis, which can increase the risk of bladder cancer if untreated, can cause hemorrhagic cystitis, the reason for Raphael's bloody urine. "It's disgusting to think about," said Raphael, who wracked her brain trying to figure out where she had become infected. One of the most famous recent outbreaks of the disease was documented in 1993 by the Centers for Disease Controland Prevention. The agency's Morbidity and Mortality Weekly Report described severe infections in two Peace Corps workers who had swum in Africa's Lake Malawi. Two weeks ago the National Institutes of Health reported that researchers have identified chemical compounds that appear promising as potential treatments for schistosomiasis, which affects 207 million people worldwide. Health officials have become increasingly concerned that the parasites will become resistant to the sole drug used to treat the illness, particularly because many cases require annual drug therapy. "Schisto is quite common in Americans overseas," said tropical medicine specialist Martin Wolfe, lead author of the MMWR report and a clinical professor at the medical schools of Georgetown and George Washington universities. Wolfe, who heads the Traveler's Medical Service, said he has treated hundreds of patients for the disease during his 45-year career, many of them affiliated with the State Department. While living in Africa years ago, Wolfe said, he saw advanced cases of the disease in which the bladder calcified and literally resembled a skull. Schistosomiasis is second only to malaria as the most devastating disease in tropical regions, according to the Atlanta-based Carter Center. In Africa alone, 100 million people are believed to be infected. Wolfe said it is not uncommon for doctors in the Washington area to see immigrants from developing countries with chronic infections, the kind Raphael had. (The disease is not contagious, and boiling water kills the parasite.) Raphael took several doses of the worm-eradicating drug praziquantel. "It's almost a magic bullet," Wolfe said. Until its advent in the mid-1970s, treatment for the infection was dangerous and sometimes harrowing, he said. Though the mystery of what caused Raphael's infection is solved, the question of how she contracted it may never be answered. Raphael said the only place she had been swimming was the Dead Sea, where snails cannot survive. Wolfe said that some patients have contracted the infection from contaminated hotel showers or stepping out of boats; it's possible, he added, that she had been infected several years earlier. Raphael's travels the year before she got sick included Kenya and Ghana, both hot spots of the infection. "The question we always ask in tropical medicine is where have you been and what have you been doing," Wolfe said. "She might not remember -- but she came into contact with freshwater somewhere." ¿ If you have a medical mystery that has been solved, e-mailmedicalmysteries@washpost.com. To read previous mysteries, visithttp://www.washingtonpost.com/health. Faith |
|
|
|
Post by bugsy on Apr 12, 2008 9:29:14 GMT -5
Well well, I'll be d**ned. After reading all of the false propoganda from primarily the CDC about there being no Schisto in the America's, low and behold A SMOKING GUN!!! It IS here and it HAS been documented. www.jaaha.org/cgi/content/abstract/37/4/349Journal of the American Animal Hospital Association, Vol 37, Issue 4, 349-355 Copyright © 2001 by American Animal Hospital Association -------------------------------------------------------------------------------- Articles Elevated parathyroid hormone-related protein and hypercalcemia in two dogs with schistosomiasis JM Fradkin, AM Braniecki, TM Craig, F Ramiro-Ibanez, KS Rogers, and DL Zoran Two adult dogs were evaluated for hypercalcemia. Diagnostic evaluation identified elevated parathyroid hormone-related protein (PTHrP) and presumptive humoral hypercalcemia of malignancy. At necropsy, schistosomiasis was diagnosed. North American schistosomiasis is caused by Heterobilharzia americana. Clinical findings may include dermatitis, coughing, diarrhea, and anorexia. Clinicopathological findings may include hypercalcemia, hyperglobulinemia, hypoalbuminemia, anemia, and eosinophilia. Diagnosis by fecal examination is difficult. Praziquantel or fenbendazole treatment may be curative or palliative. These are the first reported cases of hypercalcemia with elevated PTHrP in animals without diagnosed malignancy. Elevation of PTHrP has not been previously reported in hypercalcemic humans or in animals with granulomatous inflammation. ______________________ P.S. I feel as if I am coming back from the dead. I have been treating with Praziquantel and am beginning to feel like a human being again. I have basically been in bed most of the past year from pain and lack of energy and antihistamines......NOT today. My husband is going to have to get used to the "new" me. The lady he used to know with all the energy......hee hee. There is hope. A sidenote. Every Morg is different. We all have different life experience and could quite possible have been exposed to a variant pathogen endemic to our geographic locale. Please bear this in mind. One size does not fit all for treatment. I am just sharing what is working for me and my husband. Thanks, Faith |
|
|
|
Post by bugsy on Apr 22, 2008 17:06:55 GMT -5
Schistomes can penetrate hair follicles. www.nfid.org/publications/id_archive/skininfect.htmlInfections Associated With Hair Follicles Hair follicles serve as entry portals for a number of bacteria, although S aureus is the most common cause of localized folliculitis. A furuncle or boil begins as a localized folliculitis that slowly progresses to form an intracutaneous abscess with a pustular center. A carbuncle is composed of several contiguous furuncles. Styes and chalazions, abscesses of the eyelid, are associated with hair follicles and usually caused by S aureus. Sebaceous glands empty into hair follicles and if ducts become blocked (sebaceous cyst) may resemble staphylococcal abscesses or may become secondarily infected. Hidradenitis suppurativa can also mimic infected hair follicles particularly in the axillae. Chronic folliculitis is uncommon except in acne vulgaris where normal flora (eg, Propionibacterium acnes) plays a role. Diffuse folliculitis occurs in two distinct settings. The first, "hot-tub folliculitis" is caused by Pseudomonas aeruginosa in water insufficiently chlorinated and maintained at temperatures between 37 degrees and 40 degrees C. Infection is self-limited although bacteremia and shock have been reported. The second type of diffuse folliculitis occurs when a skin surface is exposed to water infested with freshwater avian schistosomes. Warm water and alkaline pH are suitable for the free-swimming miracidia--the intermediate host between snail and man. Miracidia readily penetrate hair follicles or pores but quickly die. These dead miracidia elicit a brisk allergic reaction causing intense itching and erythema. ______________ Faith |
|
|
|
Post by bugsy on May 7, 2008 1:39:36 GMT -5
I've had some setbacks in my Praziquantel treatments. Me and husband mistakenly only ordered thirty six, 600 mg pills during the Easter holiday. That wasn't enough for two people and a dog who have been infected for two years. Then there was a HUGE delay to recieve more because we changed to a less expensive company. It took twenty one days or so to FINALLY get them. We will both take forty two, 600 mg pills total, over time. If that doesn't make a dent in these blasted things then we will have to try another route.
I was trying 600 mg 2X's daily for five days. Great results but hubby suggested trying the 40mg/per kg body weight as suggested by the CDC and WHO. So I did tonight 5x 600mg. There are obvioulsy LESS Morg's in me this time around because I have WAY less herxing. Barely noticable. These are about $4.00 a pill. If it is a long term fix it will be well worth the cost.
Even if it isn't permanent, it is definitely a wonderful TREATMENT.
I was starting to become disfigured on my face. I had lesions all over my eyebrows and scarring. Was getting hard to fit into society looking this way. Discouraging and embarassing.
These are gone now. Just a little darkened pigment now. Just a little dab of make up to even it out and I'm good.
Husband finally got his med's yesterday. I'm excited for him. He never had the lesions however or the terrible itching like me. He was either just one of the asymtomatic ones or was just simply less infected than me.
He keeps telling me that I was just a BAD case. I'll say. ha
Best of luck to all.
Faith
|
|
|
|
Post by bugsy on May 8, 2008 6:19:00 GMT -5
I think he gets what I've been going though for the past year this morning. He started the incredible itching due to the herx from the medicine. I believe he a little taken aback as to how infected he really is. Poor guy. Am happy that he is on the road to healing, finally. It definitely affects a marriage in far reaching ways. It alters families. Faith |
|



 If it's any consolation...over 200 million are infected with this and they seem to live with it or cure it somehow. Some become more immune over thousands of years such as the Chinese. I read something the other day that said that they have gotten it under control to about a MILLION infected...a MILLION...OMG.
If it's any consolation...over 200 million are infected with this and they seem to live with it or cure it somehow. Some become more immune over thousands of years such as the Chinese. I read something the other day that said that they have gotten it under control to about a MILLION infected...a MILLION...OMG.